How Your Ear Works
Understanding the Hearing System
Quick Answer
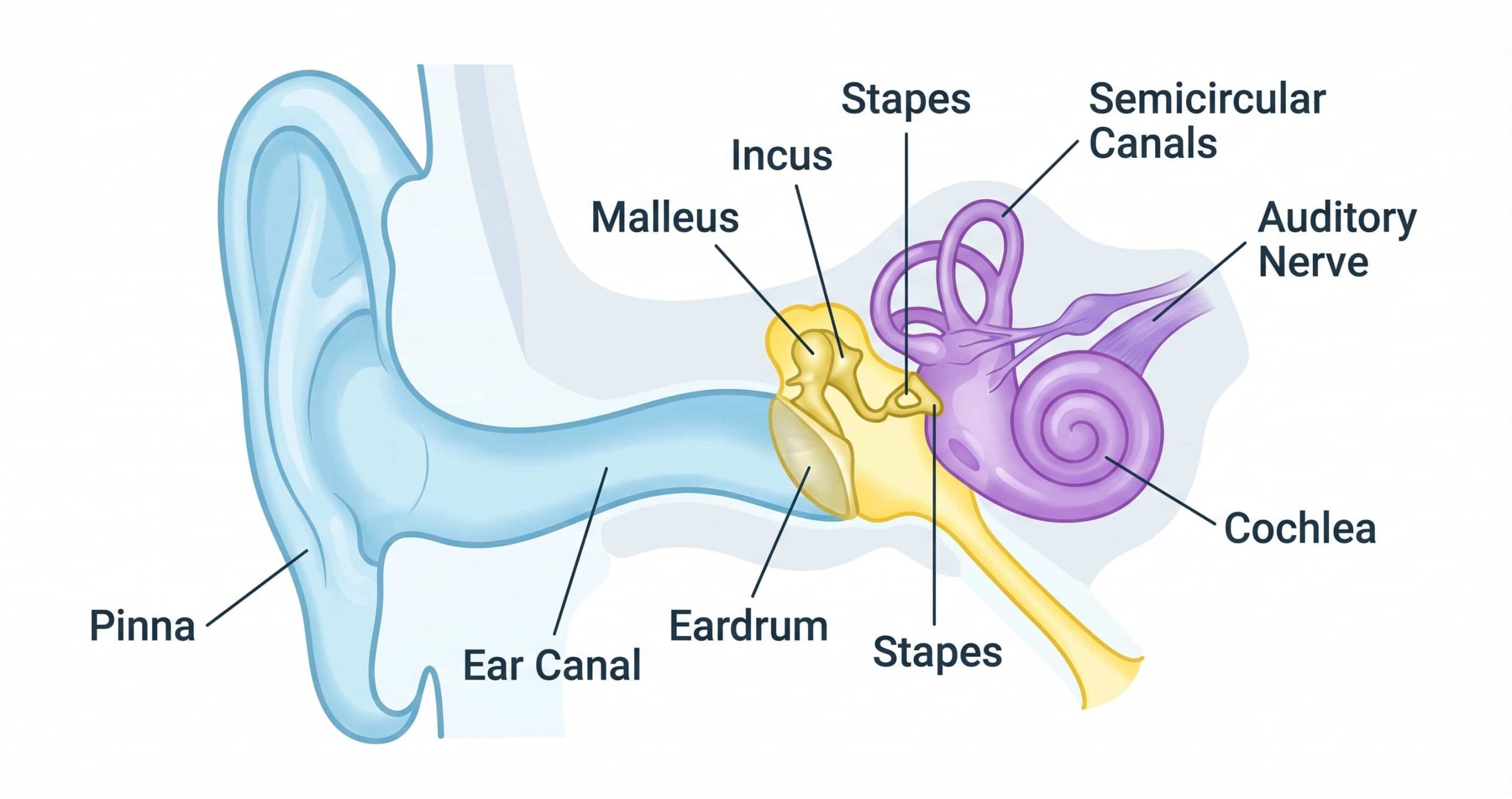
Your ear converts sound waves into electrical signals that the brain interprets as hearing. Sound enters through the outer ear (pinna and ear canal), causes the eardrum to vibrate, which moves three tiny bones in the middle ear (the ossicles). These vibrations are transmitted to the fluid-filled inner ear (cochlea), where approximately 15,000 hair cells convert the vibrations into electrical impulses. These impulses travel along the auditory nerve to the brain, where they are processed as recognisable sounds — speech, music, birdsong, or a car horn. The entire process happens in milliseconds.
Understanding how your ear works is the foundation for understanding everything about hearing — why hearing loss happens, why it affects certain sounds more than others, why hearing aids help, and why some types of hearing loss are treatable while others are not. The human ear is a remarkably elegant system that converts invisible pressure waves in the air into the rich, nuanced experience of hearing. This guide walks through that system step by step, in plain language, from the moment sound reaches your outer ear to the moment your brain recognises it as a voice, a melody, or an alarm.
The Outer Ear – Collecting Sound
The outer ear consists of two parts: the pinna (the visible part of the ear on the side of your head) and the ear canal (the tube that leads from the pinna to the eardrum).
The Pinna
The pinna is the curved, cartilage-based structure that most people think of as “the ear.” Its shape is not decorative — it is functional. The folds and contours of the pinna are designed to collect sound waves from the environment and funnel them into the ear canal. The pinna also helps your brain determine the direction a sound is coming from (sound localisation) by subtly altering the sound’s characteristics depending on whether it arrives from in front, behind, above, or below. This is why people with hearing loss in one ear often have difficulty identifying where sounds are coming from.
The Ear Canal
The ear canal is approximately 2.5 centimetres long in adults and slightly S-shaped. It serves as a passageway for sound waves to reach the eardrum, and it also provides protection — the narrow, curved shape helps prevent foreign objects from reaching the delicate structures deeper inside. The ear canal produces ear wax (cerumen), which lubricates the canal, traps dust and debris, and provides mild antibacterial protection. Under normal circumstances, ear wax migrates outward naturally. When it accumulates and forms a blockage, it can cause temporary hearing difficulty — one of the most common and easily resolved causes of conductive hearing loss.
The ear canal also acts as a resonator, naturally amplifying sounds in the 2,000–4,000 Hz frequency range — the frequencies most critical for understanding speech consonants. This natural amplification means the ear canal is not just a passive tube; it actively enhances the sounds that matter most for human communication.
The Middle Ear – Amplifying Vibrations
The middle ear is a small, air-filled space behind the eardrum. It contains the three smallest bones in the human body — collectively called the ossicles — and it serves one primary purpose: amplifying sound vibrations and transmitting them efficiently from the air-filled outer ear to the fluid-filled inner ear.
The Eardrum (Tympanic Membrane)
The eardrum is a thin, cone-shaped membrane stretched across the end of the ear canal. When sound waves reach it, the eardrum vibrates — and these vibrations precisely mirror the pattern of the incoming sound. A loud sound produces large vibrations; a soft sound produces tiny vibrations. A high-pitched sound produces rapid vibrations; a low-pitched sound produces slower vibrations. The eardrum is remarkably sensitive — it can detect vibrations smaller than the diameter of a hydrogen atom.
The Ossicles – Malleus, Incus, and Stapes
Attached to the inner surface of the eardrum are three linked bones: the malleus (hammer), incus (anvil), and stapes (stirrup). The malleus is connected to the eardrum; the incus connects the malleus to the stapes; and the stapes footplate presses against a membrane-covered opening in the cochlea called the oval window.
This chain of bones serves as a mechanical amplifier. The large surface area of the eardrum collects sound energy and concentrates it through progressively smaller bones onto the small oval window of the cochlea. The result is an amplification factor of approximately 20–30 times — essential because sound vibrations lose energy when transitioning from air (in the ear canal) to fluid (in the cochlea). Without this amplification, approximately 99.9% of sound energy would be lost at the air-fluid boundary.
When the ossicle chain is disrupted — by fluid in the middle ear, a fixated stapes (otosclerosis), or a perforated eardrum — the mechanical amplification fails and conductive hearing loss results. This type of hearing loss is often treatable because the inner ear itself is functioning normally; only the transmission mechanism is impaired.
The Eustachian Tube
The middle ear is connected to the back of the throat by the eustachian tube, which equalises air pressure on both sides of the eardrum. You experience the eustachian tube in action when your ears “pop” during altitude changes (flying, driving through mountains). When the eustachian tube is blocked — by a cold, allergies, or anatomical factors — pressure differences can build up across the eardrum, reducing its ability to vibrate freely and causing a temporary feeling of fullness or hearing reduction.
Converting Sound to Electrical Signals
The inner ear is where the mechanical miracle of hearing becomes an electrical one. It is a complex, fluid-filled structure embedded in the densest bone in the human body (the temporal bone), and it houses two separate sensory systems: the cochlea (for hearing) and the vestibular system (for balance).
The Cochlea
The cochlea is a snail-shaped, fluid-filled tube coiled approximately 2.5 turns. If you could uncoil it, it would be about 3.5 centimetres long. Running along its length is the basilar membrane, on which sit approximately 15,000 tiny sensory cells called hair cells — so named because of the microscopic hair-like projections (stereocilia) on their surfaces.
When the stapes pushes on the oval window, it creates a pressure wave in the cochlear fluid. This wave travels along the basilar membrane, which is narrow and stiff at the base (near the oval window) and wider and more flexible at the apex (the tip of the coil). Different frequencies cause the basilar membrane to vibrate maximally at different locations: high-frequency sounds activate hair cells near the base, and low-frequency sounds activate hair cells near the apex. This frequency-to-place mapping — called tonotopy — is how the cochlea sorts sound by pitch.
When the basilar membrane vibrates at a particular location, the hair cells at that location bend. This bending opens ion channels in the stereocilia, triggering an electrochemical process that converts the mechanical vibration into an electrical nerve impulse. These impulses are transmitted to the auditory nerve fibres at the base of each hair cell.
The hair cells are the critical link between mechanical sound and electrical neural signal — and they are also the most vulnerable. Once damaged by noise, ageing, medications, or disease, they do not regenerate in humans. This permanent loss of hair cells is the underlying cause of sensorineural hearing loss and most chronic tinnitus.
The Vestibular System
Adjacent to the cochlea, and sharing the same fluid space, the vestibular system detects head movement and position — providing the sense of balance. It consists of three semicircular canals (detecting rotational movement) and two otolith organs (detecting linear movement and gravity). Because the vestibular and auditory systems are so closely connected anatomically, conditions affecting the inner ear — such as Meniere’s disease — can affect both hearing and balance simultaneously.
Making Sense of Sound
The electrical impulses generated by the cochlear hair cells travel along the auditory nerve (vestibulocochlear nerve) to the brainstem, then to the auditory cortex in the temporal lobe of the brain. Along this pathway, the signal is processed through multiple relay stations where the brain begins to analyse, filter, and interpret the information.
What happens in the brain is arguably more remarkable than what happens in the ear. The auditory cortex does not just register that a sound has occurred — it identifies what the sound is (speech? music? danger?), where it is coming from (left? right? behind?), how loud it is, and what it means in context. It separates the voice of the person you are speaking with from the background noise of a busy cafe. It recognises your child’s voice in a crowd. It processes speech fast enough for you to follow a rapid conversation and respond in real time.
This processing ability depends on consistent, clear input from the ears. When hearing loss reduces the quality or quantity of auditory input, the brain receives a degraded signal — like trying to watch a television with poor reception. The brain compensates by working harder (leading to listening fatigue), filling in gaps with guesses (leading to mishearing), and sometimes generating its own signal to compensate for the missing input (leading to tinnitus).
This is why early intervention for hearing loss matters. The brain’s auditory processing pathways are “use it or lose it” systems. Prolonged auditory deprivation from untreated hearing loss can lead to neural reorganisation that makes later adjustment to hearing aids harder. Hearing aids work not just by making sounds louder — they keep the brain’s auditory pathways active and engaged.
How Hearing Loss Occurs at Each Level?
Now that you understand the hearing system, the types of hearing loss become intuitive:
- Outer ear problems (ear wax blockage, ear canal infection) → Conductive hearing loss → Often treatable with wax removal or medical treatment.
- Middle ear problems (eardrum perforation, fluid from infection, otosclerosis) → Conductive hearing loss → Often treatable with medication or surgery.
- Inner ear problems (hair cell damage from ageing, noise, medications, genetics) → Sensorineural hearing loss → Currently permanent. Managed with hearing aids or cochlear implants.
- Both outer/middle AND inner ear problems → Mixed hearing loss → Conductive component may be treatable; sensorineural component managed with amplification.
- Auditory nerve or brain processing problems → Auditory neuropathy or central auditory processing disorder → Requires specialised assessment and management.
Understanding which level is affected is why a proper hearing assessment is so important. The tests your audiologist performs are specifically designed to identify where in this system the problem lies — because the location determines the solution.
Concerned About Your Hearing?
A hearing assessment checks how well every part of your hearing system is working — from the ear canal to the cochlea. At All Ears in Hearing, we explain your results in plain language so you understand exactly what is happening and what your options are.
Frequently Asked Questions
How does the ear convert sound waves into hearing?
Sound waves enter the outer ear, travel through the ear canal, and cause the eardrum to vibrate. These vibrations are amplified by three tiny bones in the middle ear (the ossicles) and transmitted to the fluid-filled cochlea in the inner ear. Inside the cochlea, approximately 15,000 hair cells convert the vibrations into electrical impulses, which travel along the auditory nerve to the brain. The brain then processes these impulses as recognisable sounds. The entire process takes just milliseconds.
What are the three parts of the ear?
The ear has three main parts: the outer ear (pinna and ear canal, which collect and channel sound), the middle ear (eardrum and three ossicle bones, which amplify vibrations), and the inner ear (cochlea, which converts vibrations into electrical signals sent to the brain). Each part plays a specific role in the hearing process, and problems at any level can cause different types of hearing loss.
What are cochlear hair cells and why are they important?
Cochlear hair cells are approximately 15,000 tiny sensory cells lining the basilar membrane inside the cochlea. They are the critical link between mechanical sound vibration and electrical nerve signals. When sound causes the basilar membrane to vibrate, the hair cells bend and generate electrical impulses that are sent to the brain via the auditory nerve. Hair cells are fragile and cannot regenerate once damaged — their loss is the primary cause of permanent sensorineural hearing loss.
Why does the ear also affect balance?
The inner ear houses two systems: the cochlea (for hearing) and the vestibular system (for balance). The vestibular system consists of three semicircular canals and two otolith organs that detect head movement and position. Because these systems share the same anatomical space and fluid, conditions affecting the inner ear — such as Meniere’s disease, labyrinthitis, or BPPV — can affect both hearing and balance simultaneously.
What is the smallest bone in the human body?
The stapes (stirrup) in the middle ear is the smallest bone in the human body, measuring approximately 3 millimetres in height. Along with the malleus (hammer) and incus (anvil), the stapes forms the ossicle chain that amplifies and transmits sound vibrations from the eardrum to the cochlea. Despite its tiny size, the stapes plays a critical role in hearing — conditions like otosclerosis, which restrict the stapes’ movement, can cause significant conductive hearing loss.
Sources and References
- Audiology Australia — Professional Practice Resources
- National Institute on Deafness and Other Communication Disorders (NIDCD) — How Do We Hear?
- World Health Organization — World Report on Hearing (2021)
- Purves et al. — Neuroscience (6th edition) — Auditory System chapters
This article is intended as general health information. A hearing assessment with a qualified audiologist is recommended for anyone with concerns about their hearing. Information current as of April 2026.