Types of Hearing Loss Explained Sensorineural, Conductive and Mixed
Quick Answer
There are three main types of hearing loss: sensorineural (damage to the inner ear or auditory nerve — the most common type, accounting for approximately 90% of cases), conductive (a problem in the outer or middle ear that blocks sound transmission — often treatable or reversible), and mixed (a combination of both). A hearing assessment is the only way to determine which type you have, as this directly affects which management approach is most appropriate.
Table of Contents
Understanding the type of hearing loss you have is just as important as knowing the degree. Two people with the same level of hearing difficulty may have completely different underlying causes — and therefore very different treatment pathways. One may benefit from a straightforward medical intervention that restores hearing to near-normal levels. The other may require hearing aids as a long-term management strategy. The type of hearing loss determines which pathway is appropriate, which is why a proper diagnostic hearing assessment matters so much more than an online screening or a gut feeling about what is happening.
This guide explains the three types of hearing loss in plain language, covers what causes each one, whether it can be reversed, and what management options exist. If you are reading this because you have noticed changes in your hearing — or because someone you care about has — this is the right place to start building your understanding.
How Hearing Loss Is Classified
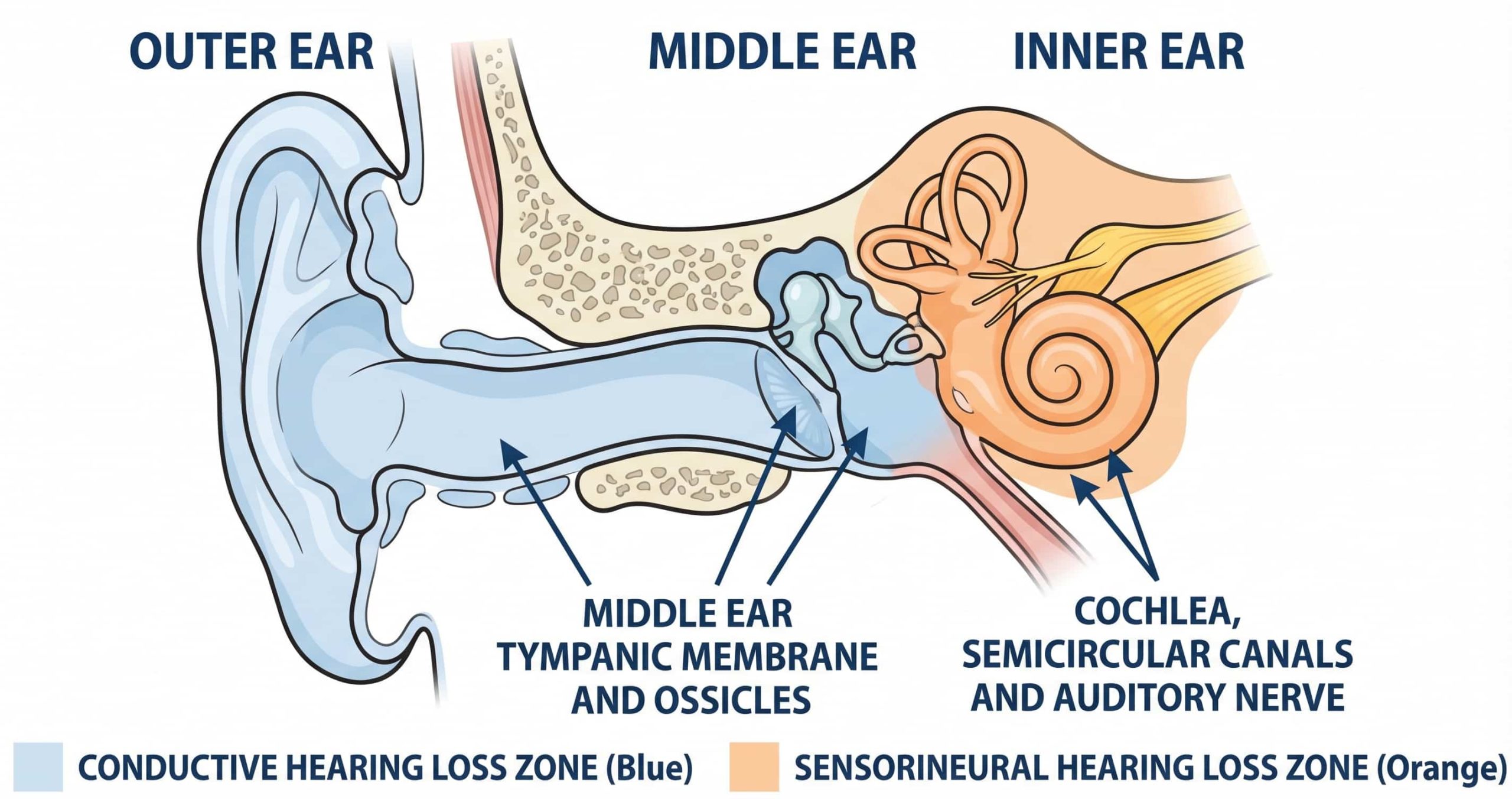
Hearing loss is classified based on where in the auditory system the problem occurs. Sound travels through your ear in a specific pathway: from the outer ear (pinna and ear canal), through the middle ear (eardrum and three tiny bones called the ossicles), into the inner ear (cochlea), and along the auditory nerve to the brain. A problem at any point along this pathway can cause hearing loss, and the location of the problem determines the type.
- Outer or middle ear problem → Conductive hearing loss
- Inner ear or auditory nerve problem → Sensorineural hearing loss
- Both locations affected → Mixed hearing loss
Your audiologist determines which type you have through a combination of tests during your hearing assessment, including air conduction testing (sound delivered through headphones), bone conduction testing (sound delivered through a vibrator placed behind the ear, bypassing the outer and middle ear), and tympanometry (measuring middle ear function). The relationship between these results reveals exactly where the problem lies.
Sensorineural Hearing Loss
Sensorineural hearing loss (SNHL) is the most common type of hearing loss, accounting for approximately 90% of all hearing loss in adults. It occurs when the hair cells in the cochlea (inner ear) are damaged or when the auditory nerve that carries signals to the brain is impaired. Once these delicate hair cells are damaged, they do not regenerate — which is why sensorineural hearing loss is currently considered permanent and irreversible in the vast majority of cases.
Common Causes of Sensorineural Hearing Loss
- Ageing (presbycusis): The most common cause. Age-related hearing loss develops gradually, typically affecting high-frequency sounds first — which is why consonants like “s”, “f”, and “th” often become harder to hear before vowels do.
- Noise exposure: Prolonged or repeated exposure to sounds above 85 decibels — from occupational noise, concerts, power tools, or personal audio devices at high volume — causes cumulative damage to cochlear hair cells.
- Genetics: Family history of hearing loss increases the risk. Some genetic conditions cause hearing loss from birth (congenital) or progressive loss that develops later in life.
- Ototoxic medications: Certain drugs — including some antibiotics, chemotherapy agents, and high-dose aspirin — can damage the cochlea or auditory nerve.
- Head trauma: Injury to the head or temporal bone can damage the inner ear structures.
- Viral infections: Some viral illnesses — including measles, mumps, and meningitis — can cause sensorineural hearing loss.
- Meniere’s disease: A condition affecting the inner ear that causes fluctuating hearing loss, vertigo, and tinnitus.
Can Sensorineural Hearing Loss Be Reversed?
In the vast majority of cases, no. Sensorineural hearing loss is currently permanent because the damaged hair cells in the cochlea cannot regenerate with present medical technology. Research into hair cell regeneration and gene therapy is ongoing and represents a promising area of future treatment, but as of April 2026, no approved treatment exists that can restore cochlear hair cells in humans. The most effective management for sensorineural hearing loss is hearing aids, which amplify sound to compensate for the reduced sensitivity of the damaged hair cells. For severe to profound sensorineural hearing loss where hearing aids no longer provide sufficient benefit, cochlear implants may be appropriate.
The one notable exception is sudden sensorineural hearing loss (SSHL), which may respond to medical treatment — typically corticosteroids — if treatment is initiated within 24–72 hours of onset. This is why sudden hearing loss is treated as a medical emergency.
Conductive Hearing Loss
Conductive hearing loss occurs when sound cannot pass efficiently through the outer ear canal, eardrum, or middle ear bones to reach the inner ear. The inner ear and auditory nerve are functioning normally — the problem is purely mechanical. Because the underlying cause is often a physical blockage or structural issue, conductive hearing loss is frequently treatable and sometimes fully reversible.
Common Causes of Conductive Hearing Loss
- Ear wax blockage: Impacted cerumen is one of the most common and most easily resolved causes. Professional ear wax removal often restores hearing immediately.
- Middle ear infections (otitis media): Fluid accumulation in the middle ear from infection reduces the eardrum’s ability to vibrate. In children, glue ear (otitis media with effusion) is a particularly common cause of temporary conductive hearing loss.
- Eardrum perforation: A hole in the eardrum — from infection, trauma, or sudden pressure changes — reduces sound transmission.
- Otosclerosis: Abnormal bone growth around the stapes (the smallest bone in the middle ear) progressively fixes the bone in place, preventing it from transmitting vibrations effectively. Otosclerosis can be treated surgically (stapedectomy) or managed with hearing aids.
- Outer ear conditions: Conditions such as swimmer’s ear (otitis externa), bony growths in the ear canal (exostoses), or congenital abnormalities of the outer ear can block sound transmission.
- Eustachian tube dysfunction: When the eustachian tube — which connects the middle ear to the back of the throat — is blocked or not functioning properly, pressure changes in the middle ear can reduce hearing.
Can Conductive Hearing Loss Be Reversed?
In many cases, yes. Because conductive hearing loss involves a mechanical problem rather than nerve damage, addressing the underlying cause often restores hearing. Ear wax removal, treatment of middle ear infections, surgical repair of a perforated eardrum, or a stapedectomy for otosclerosis can all result in significant hearing improvement. However, not all conductive hearing loss is reversible — chronic middle ear disease, for example, may cause permanent structural changes. A thorough assessment by an audiologist and, where appropriate, referral to an ENT specialist is the best way to determine whether your conductive hearing loss is treatable.
Mixed Hearing Loss
Mixed hearing loss is exactly what the name suggests: a combination of sensorineural and conductive hearing loss occurring simultaneously. The person has an underlying permanent sensorineural component (inner ear or nerve damage) along with an additional conductive component (outer or middle ear issue) on top of it.
A common example is an older adult with age-related sensorineural hearing loss who also develops impacted ear wax or a middle ear infection. The sensorineural component is permanent, but the conductive component may be treatable — and treating the conductive portion often produces a noticeable improvement in hearing, even though it cannot address the underlying sensorineural loss.
Mixed hearing loss is identified during audiometric testing when both air conduction and bone conduction thresholds are elevated, with an air-bone gap indicating the conductive component. Management typically involves addressing the treatable conductive element first (through medical treatment, ear wax removal, or surgery), followed by hearing aids if significant sensorineural hearing loss remains.
How Do You Know Which Type of Hearing Loss You Have?
You cannot determine the type of hearing loss from symptoms alone. Someone with conductive hearing loss from ear wax and someone with sensorineural hearing loss from ageing may both experience muffled hearing, difficulty following conversations, and the need to increase the television volume. The subjective experience can be similar even though the underlying cause — and therefore the appropriate management — is completely different.
A comprehensive hearing assessment at a qualified audiology clinic is the only reliable way to determine your type of hearing loss. The assessment includes specific tests designed to differentiate between conductive and sensorineural components:
- Air conduction audiometry: Measures your hearing thresholds through headphones (sound travels through the outer and middle ear)
- Bone conduction audiometry: Measures your inner ear function directly by sending sound vibrations through the skull, bypassing the outer and middle ear
- The air-bone gap: The difference between these two results reveals whether a conductive component is present. If air conduction is worse than bone conduction, a conductive problem is contributing to the hearing loss
- Tympanometry: Measures how the eardrum and middle ear respond to pressure changes, helping identify middle ear fluid, eustachian tube dysfunction, or eardrum perforation
At All Ears in Hearing, Brad and Rachel’s team conducts all of these tests as part of a standard hearing assessment at our Rochedale South and Shailer Park clinics. Understanding your audiogram results is an important part of the process, and we take the time to explain what every result means in plain language.
Management Options by Type
Sensorineural Hearing Loss Management
- Hearing aids — the primary management for mild to severe sensorineural hearing loss. Modern hearing aids are precisely programmed to your individual audiogram and can significantly improve speech understanding and quality of life.
- Cochlear implants — for severe to profound sensorineural hearing loss where hearing aids no longer provide sufficient benefit. Cochlear implant candidacy is assessed through a specialised evaluation process.
- Assistive listening devices — FM systems, telecoils, and other devices that supplement hearing aids in specific listening situations.
- Communication strategies — practical techniques that help you and the people around you communicate more effectively.
Conductive Hearing Loss Management
- Medical treatment — antibiotics for ear infections, decongestants for eustachian tube dysfunction, or other targeted treatments depending on the cause.
- Ear wax removal — professional microsuction for impacted cerumen.
- Surgery — tympanoplasty for eardrum repair, stapedectomy for otosclerosis, or grommets for chronic middle ear fluid. Surgical options are managed by ENT specialists.
- Hearing aids — if the conductive component cannot be fully resolved through treatment or surgery, hearing aids can amplify sound to overcome the mechanical barrier.
Mixed Hearing Loss Management
- Treat the conductive component first — address the reversible element through appropriate medical or surgical intervention.
- Hearing aids for the remaining sensorineural component — once the conductive issue is resolved, hearing aids can be fitted to manage the permanent inner ear component.
Find Out What Type of Hearing Loss You Have
A comprehensive hearing assessment at All Ears in Hearing will identify your specific type and degree of hearing loss and determine the most appropriate management pathway. Our audiologists are not paid commission — the recommendation you receive is based entirely on your clinical needs.
Frequently Asked Questions
What are the three types of hearing loss?
The three types are sensorineural (inner ear or auditory nerve damage — the most common, accounting for approximately 90% of cases), conductive (a problem in the outer or middle ear that blocks sound transmission), and mixed (a combination of both sensorineural and conductive hearing loss occurring together). Each type has different causes and different management approaches, which is why a professional hearing assessment is essential for determining the correct pathway.
Which type of hearing loss is permanent?
Sensorineural hearing loss is generally permanent because the damaged hair cells in the inner ear cannot currently regenerate. It can be effectively managed with hearing aids or, in severe cases, cochlear implants. Conductive hearing loss is often treatable or reversible depending on the underlying cause — for example, ear wax removal or treatment of a middle ear infection may fully restore hearing. Mixed hearing loss involves both a permanent sensorineural component and a potentially treatable conductive component.
What is the most common type of hearing loss?
Sensorineural hearing loss is the most common type, accounting for approximately 90% of all hearing loss cases. The most frequent causes are age-related changes (presbycusis) and noise exposure. It is managed primarily with hearing aids, which amplify sound to compensate for the reduced sensitivity of the damaged hair cells in the inner ear.
How can I tell if my hearing loss is conductive or sensorineural?
You cannot reliably distinguish between conductive and sensorineural hearing loss based on symptoms alone. Both types can produce similar experiences such as muffled hearing and difficulty following conversation. A professional hearing assessment that includes both air conduction and bone conduction testing is required to differentiate the types. The difference between these two measurements (the air-bone gap) reveals whether a conductive component is present.
Can conductive hearing loss be fixed?
In many cases, yes. Because conductive hearing loss involves a mechanical or structural issue in the outer or middle ear rather than nerve damage, addressing the cause often restores hearing. Professional ear wax removal, treatment of middle ear infections, surgical repair of a perforated eardrum, or surgery for otosclerosis can all result in significant hearing improvement. However, not all conductive hearing loss is reversible — chronic middle ear disease or structural abnormalities may require ongoing management with hearing aids. An audiologist and, where appropriate, an ENT specialist can determine the best approach for your specific situation.
Sources and References
- World Health Organization — World Report on Hearing (2021)
- Audiology Australia — Clinical Practice Standards
- Australian Institute of Health and Welfare — Hearing health data
- National Institute on Deafness and Other Communication Disorders (NIDCD)
Individual results may vary. A comprehensive hearing assessment is required to determine the type and degree of your hearing loss and the most appropriate management approach. Information current as of April 2026.